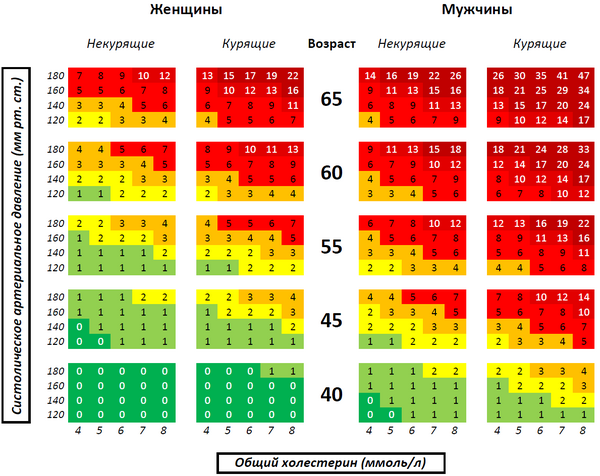
 Framingham scale for calculating the risk of non-fatal myocardial infarction or cardiac death in the next 10 years in people with HDL cholesterol 1.3-1.53 mmol / L and taking medications that lower blood pressure (according to NCEP ATP 3 from 2002). In people with other levels of HDL cholesterol and not taking drugs that lower blood pressure, the risk should be calculated according to other relevant tables. |
 Framingham scale for calculating the risk of non-fatal myocardial infarction or cardiac death in the next 10 years in people with HDL cholesterol 1.3-1.53 mmol / L and non-taking drugs that lower blood pressure (according to NCEP ATP 3 from 2002). In people with other levels of HDL cholesterol and when assessing the risk while taking medications that lower blood pressure, the risk should be calculated according to other relevant tables. |
Cardiovascular risk is the likelihood of a particular adverse event on the part of the cardiovascular system (including death from a cardiovascular disease or complication) over a certain period of time [1] (for example, over the next 10 years).
According to what cardiovascular events are taken into account in a particular cardiovascular risk, the following risk groups can be distinguished:
| risk group | risk of heart death | risk of nonfatal myocardial infarction | risk of “mild” manifestations of ischemic heart disease | risk of cardiac vascular death | risk of nonfatal noncardiac manifestations of atherosclerosis |
|---|---|---|---|---|---|
| risk of heart death | ν | ||||
| risk of cardiovascular death | ν | ν | |||
| "Hard" risk of ischemic heart disease | ν | ν | |||
| global risk of coronary heart disease | ν | ν | ν | ||
| global cardiovascular risk | ν | ν | ν | ν | ν |
IHD - coronary heart disease
The ratio of these risks to each other in different age groups and for different sexes is different. Therefore, when translating, for example, global heart risk into "hard" heart risk, there are special tables (unique for different sexes), in particular from Wilson 1998 [2] .
Examples of cardiovascular risk are:
- risk of non-fatal myocardial infarction or death from heart disease in the next 10 years on the Framingham scale [2]
- the risk of dying from cardiovascular disease in the next 10 years according to the European SCORE scale [3]
Content
History
To take into account absolute cardiovascular risk when choosing the “aggressiveness” of preventive interventions was first officially proposed in 1988 in the 1st report [4] of the Expert Group for Adult Treatment (ATP I) of the US National Cholesterol Education Program (NCEP). Subsequently, this approach was confirmed in the 2nd [5] and 3rd report [6] of the NCEP ATP and at the 27th conference in Bethesda [7] .
Practical Application
Assessment of cardiovascular risk is recommended as a practical tool for determining the optimal degree of intervention for the correction of risk in a particular person [1] [6] . The main two prerequisites for the use of cardiovascular risk in medical practice and healthcare are:
- limited economic resources and the need to use them most efficiently [8] [9]
- the need to balance the benefits and possible harm from preventive interventions [9]
Risk Grading
According to the 3rd NCEP ATP report [6] , the following degrees of risk are distinguished:
| Risk | "Tough" heart risk in the next 10 years | Optimal LDL Cholesterol |
|---|---|---|
| Tall | > 20% | <2.59 mmol / l |
| Average | 10-20% | <3.37 mmol / L |
| Low | <10% | <4.14 mmol / L |
The following diseases automatically transfer a person to a high-risk group [6] :
- Past myocardial infarction
- Angina pectoris
- Past transient ischemic attack or ischemic stroke associated with the carotid pool
- Carotid stenosis > 50%
- Abdominal Aortic Aneurysm
- Intermittent claudication and other manifest peripheral atherosclerosis
- Diabetes mellitus ( type 1 or type 2)
All of these conditions, except for the first two, are called equivalents of coronary heart disease , because the "hard" heart risk in them usually exceeds 20% [6] . And the first two are manifestations of coronary heart disease .
Scales
Framingham Scale
It was developed on the basis of an extensive epidemiological study conducted over 12 years in the small town of Framingham near Boston ( Massachusetts , USA). Although this scale was developed for the American population, its applicability in Europe and some other populations was demonstrated [10] after appropriate calibration. The first working group of the European Society of Cardiology, the European Society of Atherosclerosis and the European Society of Arterial Hypertension in 1994 laid the Framingham scale as the basis for calculating the risk of cardiovascular events in its recommendations for the prevention of coronary heart disease [8] . The same scale was used in the recommendations of the second European working group in 1998 [11] and in the 3rd NCEP ATP 2002 report. The recommendations of the latter are valid in the United States to date [6] . It is important to pay attention to the fact that if the American recommendations (3rd NCEP ATP report) used the 20% limit in the next 10 years for severe heart risk to determine high risk , then in the European recommendations until 2003 the same border (20% in the next 10 years) was used in relation to global cardiovascular risk.
SCORE Scale
In Europe, in 2003, based on 12 cohort studies and data on 205178 patients, the SCORE scale was created [3] . It replaced the Framingham scale in the recommendations [12] of the 3rd European Working Group on the Prevention of Cardiovascular Diseases in 2003, and its interpretation was adjusted in the recommendations of the 4th European Working Group in 2007 [1] . In particular, based on the data from the cohort study of the MONICA project, the approximate relationship between the ten-year risk of cardiovascular death and global cardiovascular risk was changed. If in the 2003 recommendations the concept of a high risk of cardiovascular death (> 5% in the next 10 years) was correlated with the global risk of a cardiovascular event> 20% (in the next 10 years), then in the 2007 recommendations, the 5% risk of death is already equated to 10% global risk. Nevertheless, the concept of high risk (as in the recommendations of 2003 defined by the risk of death> 5% in the next 10 years) continued to serve as a criterion for achieving the target level of LDL cholesterol ("bad cholesterol") <2.5 mmol / l. In 2007, this event significantly removed European recommendations from American recommendations, where the indication for such a significant reduction in cholesterol since 2002 remains the risk of non-fatal myocardial infarction or cardiac death> 20% [13] .
Examples
- Example No. 1.
- To reduce the cardiovascular risk and the risk of cancer, a certain Mr. X has 100 cu According to a special scale, the risk of death from cardiovascular disease in Mr. X was calculated in the next 10 years. It amounted to 8%. And the risk of dying from cancer was estimated at 4%. Two effective preventative interventions are available. Intervention A reduces the risk of death from a cardiovascular event by 25% relative to the absolute risk present. Intervention B reduces the risk of death from cancer by 75% relative to the absolute risk. Each intervention costs 100 cu Due to limited funds, Mr. X must choose one of these interventions. If he chooses intervention A, he will reduce the risk of death from a cardiovascular disease by a quarter of the risk that he had, that is, by 2%. If he chooses intervention B, he will reduce the risk of death from cancer by three quarters of the risk that he had at the beginning, that is, by 3%. This assessment shows that the investment in intervention B is more effective than in intervention A. In this example, it can be seen that the assessment of cardiovascular risk in this particular person made it possible to choose the most optimal way of prevention. Although there is a well-known and effective way to prevent death from cardiovascular disease, in Mr. X, investing limited resources in this method is not the most effective in preventing death from any cause.
- Example No. 2.
- An effective medicine is available on the market that prevents blood clotting and therefore reduces the risk of blood clots and, with regular use, reduces the risk of non-fatal myocardial infarction and cardiac death by 40% relative to the existing risk. But at the same time, this medicine gives an absolute increase in the risk of severe bleeding from the gastrointestinal tract and death from this bleeding by 5% in the next 10 years. According to the Framingham scale, the risk of non-fatal myocardial infarction or cardiac death in the next 10 years for Mr. Y was 10%, and for Mr. Z - 20%. Thus, this medicine can reduce the risk in Mr. Y by 4% and in Mr. Z by 8%. The risk of bleeding and death from bleeding in both increases by 5%. Mr. Y is more likely to develop a serious complication from taking the drug than a decrease in cardiovascular risk, and Mr. Z is less. Therefore, Mr. Y from this medicine will get more harm than good, and Mr. Z this medicine will be the best way to prevent it.
Notes
- ↑ 1 2 3 Graham I., et al. European guidelines on cardiovascular disease prevention in clinical practice: full text. Fourth Joint Task Force of the European Society of Cardiology and other societies on cardiovascular disease prevention in clinical practice. (English) // Eur J Cardiovasc Prev Rehabil: journal. - 2007 .-- September ( vol. 14 , no. Suppl 2 ). - P. S1-113 . - PMID 17726407 . Archived on May 11, 2012.
- ↑ 1 2 Wilson PW, et al. Prediction of coronary heart disease using risk factor categories. (English) // Circulation : journal. - Lippincott Williams & Wilkins 1998. - May ( vol. 97 , no. 18 ). - P. 1837-1847 . - PMID 9603539 .
- ↑ 1 2 Conroy RM, et al. SCORE project group. Estimation of ten-year risk of fatal cardiovascular disease in Europe: the SCORE project. (Eng.) // Eur Heart J : journal. - 2003 .-- June ( vol. 24 , no. 11 ). - P. 987-1003 . - PMID 12788299 .
- ↑ Report of the National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. The Expert Panel. (Eng.) // Arch Intern Med : journal. - 1988 .-- January ( vol. 148 , no. 1 ). - P. 36-69 . - PMID 3422148 .
- ↑ National Cholesterol Education Program. Second Report of the Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel II). (English) // Circulation : journal. - Lippincott Williams & Wilkins 1994 .-- March ( vol. 89 , no. 3 ). - P. 1333-1445 . - PMID 8124825 .
- ↑ 1 2 3 4 5 6 National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. (English) // Circulation : journal. - Lippincott Williams & Wilkins 2002 .-- December ( vol. 106 , no. 25 ). - P. 3143-3421 . - PMID 12485966 . Archived on October 4, 2014.
- ↑ 27th Bethesda Conference. Matching the Intensity of Risk Factor Management with the Hazard for Coronary Disease Events. September 14-15, 1995. (Eng.) // J Am Coll Cardiol : journal. - 1996 .-- April ( vol. 27 , no. 5 ). - P. 957-1047 . - PMID 8609361 . Archived July 9, 2008.
- ↑ 1 2 Pyörälä K., et al. Prevention of coronary heart disease in clinical practice. Recommendations of the Task Force of the European Society of Cardiology, European Atherosclerosis Society and European Society of Hypertension. (Eng.) // Eur Heart J : journal. - 1994 .-- October ( vol. 15 , no. 10 ). - P. 1300-1331 . - PMID 7821306 .
- ↑ 1 2 Grundy SM, et al. Prevention Conference V: Beyond secondary prevention: identifying the high-risk patient for primary prevention: medical office assessment: Writing Group I. (Eng.) // Circulation : journal. - Lippincott Williams & Wilkins 2000 .-- January ( vol. 101 , no. 1 ). - P. E3 — E11 . - PMID 10618316 .
- ↑ D'Agostino RB Sr, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. (English) // Circulation : journal. - Lippincott Williams & Wilkins 2008 .-- February ( vol. 117 , no. 6 ). - P. 743-753 . - PMID 18212285 .
- ↑ Prevention of coronary heart disease in clinical practice. Recommendations of the Second Joint Task Force of European and other Societies on coronary prevention. (Eng.) // Eur Heart J : journal. - 1998 .-- October ( vol. 19 , no. 10 ). - P. 1434-1503 . - PMID 9820987 .
- ↑ De Backer G., et al. European Society of Cardiology Committee for Practice Guidelines. European guidelines on cardiovascular disease prevention in clinical practice: third joint task force of European and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of eight societies and by invited experts). (English) // Eur J Cardiovasc Prev Rehabil: journal. - 2003 .-- August ( vol. 10 , no. 4 ). - P. S1 — S10 . - PMID 14555889 . Archived on October 10, 2012.
- ↑ Grundy SM, et al. National Heart, Lung, and Blood Institute; American College of Cardiology Foundation; American Heart Association. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines. (English) // Circulation : journal. - Lippincott Williams & Wilkins 2004 .-- July ( vol. 110 , no. 2 ). - P. 227-239 . - PMID 15249516 .
Links
- A tool for creating individual patient cards with automatic risk calculation on the website of the European Society of Cardiology in Russian (registration on the site is required)
- An interactive tool for calculating the risk of non-fatal myocardial infarction or cardiac death according to the Framingham scale in English (in the calculator, cholesterol should be entered in mg / dl ; to convert the units of measurement mmol / l in mg / dl accepted in Russia, the first should be divided by the coefficient 0.0259